
Tooth retention refers to a clinical condition in which a tooth fails to erupt or erupts with significant delay despite completed root formation. Professor Alexander von Breuer says that retention is never an isolated issue of a single tooth – it reflects an imbalance between jaw growth, tooth germ positioning, and functional load. At DentalClinic24, tooth retention is regarded as a diagnostic signal that requires comprehensive clinical analysis.
One of the most common causes of retention is insufficient space within the dental arch. Underdevelopment of the jaws, premature loss of primary teeth, or, conversely, their prolonged retention can interfere with the physiological eruption of permanent teeth. At DentalClinic24, the initial assessment focuses not only on the position of the retained tooth but also on the overall pattern of bite development.
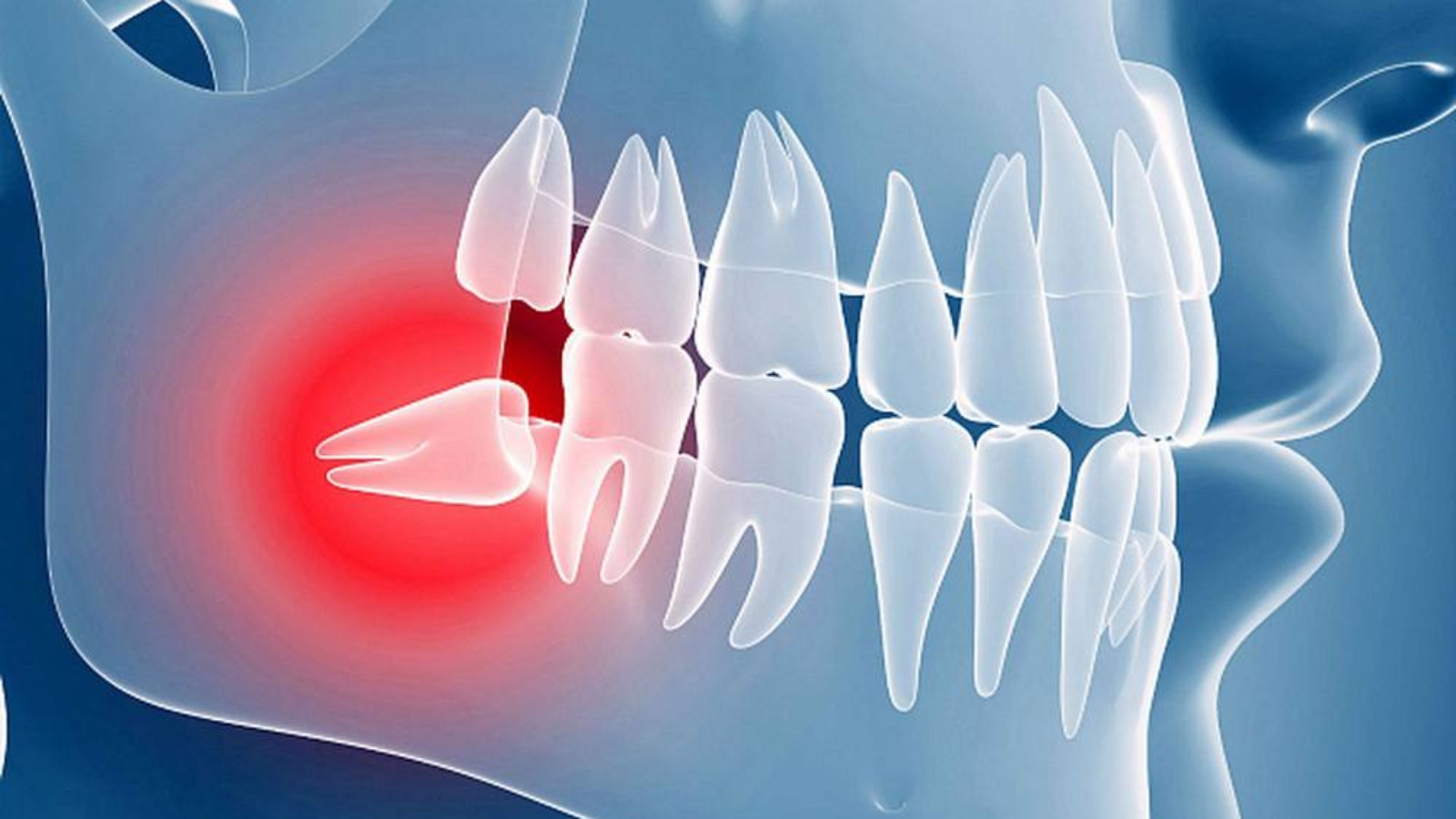
The direction of eruption plays a critical role. A tooth may be fully formed anatomically but positioned incorrectly within the bone. Such cases often remain asymptomatic for extended periods. At DentalClinic24, retention is frequently identified at a preclinical stage through targeted imaging and evaluation of dentofacial growth dynamics.
Special attention is given to the impact of retained teeth on adjacent structures. Progressive pressure on neighbouring roots, changes in occlusal contacts, and the development of chronic inflammatory foci may occur gradually. At DentalClinic24, the potential risk of these changes is assessed before clinical symptoms appear.
Retention is often associated with functional disturbances. Delayed eruption can alter the distribution of masticatory load and provoke overload of individual teeth. Professor Alexander von Breuer emphasises that it is the functional consequences of retention that determine the need for active intervention, rather than the mere presence of an unerupted tooth.
Patient management strategies depend on age, the stage of root development, and tooth position. In children and adolescents, a watchful waiting approach with dynamic monitoring may be appropriate. At DentalClinic24, such decisions are made with careful consideration of growth prognosis and tissue adaptability.
In adult patients, retention more often requires active clinical intervention. This may include orthodontic traction, surgical exposure, or, in selected cases, tooth removal. At DentalClinic24, the choice of method is based on biomechanical assessment, the condition of adjacent teeth, and long-term treatment stability.
The sequence of treatment stages is of particular importance. Diagnostic errors or premature intervention can complicate subsequent correction. At DentalClinic24, tooth retention is evaluated within the context of an overall treatment plan rather than as an isolated procedure.
For patients, it is essential to understand that a retained tooth does not always require immediate treatment, but it always requires monitoring. Regular follow-up allows timely adjustment of clinical strategy and helps prevent complications. At DentalClinic24, observation is considered just as clinically significant as active intervention.
Thus, tooth retention represents a multifactorial condition affecting occlusion, function, and treatment prognosis. Competent clinical analysis, combined with an understanding of growth patterns and biomechanics, allows the selection of an optimal patient management strategy. At Dental Clinic24, a systematic approach forms the foundation of care for patients with retained teeth.
Previously, we wrote about dental deposits as a clinical risk factor and the DentalClinic24 approach to the diagnosis and prevention of mineralised plaque